What may indicate a violation of tendon reflexes. Rubric "Tendon
Skin reflexes spinal cord are caused by dashed skin irritation, in response to which a contraction of one or another muscle or group of them occurs. Unlike tendon reflexes cutaneous are not congenital. They occur in children different ages(from 5 months to 3 years). Obviously, their formation is largely due to the development of the cerebral cortex and pyramidal pathways. The double circuit of skin reflexes (in the spinal cord and cerebral cortex) is due to the fact that their absence can be caused by damage to both their spinal reflex arc and the pyramidal pathway, which is an essential link in the efferent part of the skin reflex arc.
Skin reflexes include:
Abdominal reflexes. They are caused by rapid stroke irritation of the skin of the abdomen with the blunt end of the needle or the handle of the hammer. The response consists in contraction of the abdominal muscles on the side of the same name. To evoke the upper abdominal reflex, the stroke irritation is applied on the skin parallel to the costal arch, for the middle abdominal reflex - at the level of the navel in the horizontal direction, for the lower abdominal reflex - parallel to the inguinal fold.
This also includes the bone-abdominal reflex described by V. M. Bekhterev, which consists in the fact that when a hammer strikes the edge of the costal arch medially from the nipple line, the abdominal muscles of the corresponding side contract. These deep (periosteal) abdominal reflexes can be used to compare abdominal reflexes on either side.
Cremaster muscle reflex is caused by applying dashed irritation to the skin of the inner surface of the thigh 1-2 cm below the inguinal fold. The response in this case is expressed in pulling the testicle up.
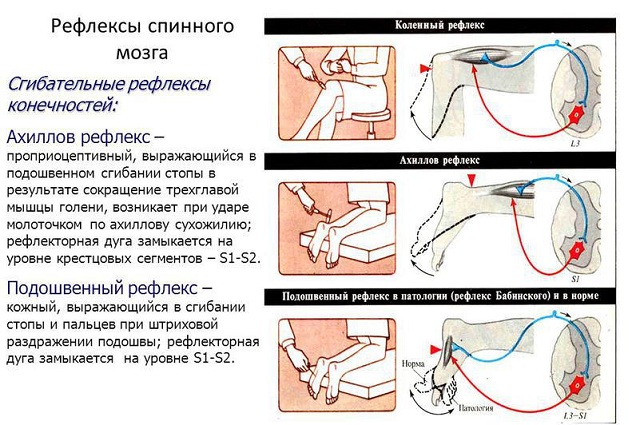
plantar reflex It is caused by a stroke irritation of the sole, in response to which plantar flexion of the fingers follows.
anal reflex caused by a prick of the skin anus. In response, its circular muscle contracts.
A special place is occupied by the so-called articular reflexes. In their essence, they belong to deep reflexes, however, they are similar to skin reflexes. late appearance and dependence on the pyramidal pathways. With the integrity of the spinal reflex arcs of the articular reflexes, their weakening or disappearance is regarded as a sign of damage to the pyramidal tracts. These include the following reflexes.
Mayer's reflex. It is caused by forced flexion of the main phalanx of the III or IV finger of the supinated hand. In this case, flexion of the main phalanx occurs, as well as adduction and extension of the nail phalanx. thumb.
Reflex Leri. In the position of the supinated hand and bent fingers, vigorous flexion of the fingers and hand in the wrist joint is performed. In this case, there is a reflex flexion of the arm in elbow joint.
A decrease or absence of skin and articular reflexes, combined with an increase in tendon reflexes and the appearance of pathological ones, is a reliable sign of damage to the pyramidal tracts. It should be borne in mind that abdominal reflexes are often not evoked if the patient has a flabby abdominal wall with complete intactness of the reflex arcs of these reflexes.
An increase in skin reflexes does not play such a role in the clinic as their decrease or absence. An increase in abdominal and plantar reflexes is often found in functional diseases. nervous system, at general increase her excitability. Usually, in these patients, the study of reflexes itself causes a general emotional reaction (trembling of the whole body, screaming, etc.).
Of some importance in the clinic is an increase in the Mayer articular reflex. It is manifested by the fact that the thumb is adducted and opposed with the slightest flexion of the main phalanges of the III and IV fingers, and also by the fact that additional contractions of the flexors of the forearm and deltoid muscle are caused. An increase in the reflex is sometimes observed with frontal localizations of the process, and on the side of the same name to the focus. Often, an increase in the Mayer reflex accompanies the grasping reflex.
The most important tendon reflex in the lower extremities is knee, or patellar. In this reflex, stimulation of the tendon of the quadriceps femoris causes its contraction.
The method of obtaining it is as follows: the patient sits down and crosses his legs, and the examiner strikes the lig with a hammer. patellae proprium. Due to the reflex contraction of the quadriceps femoris muscle, the lower leg swings forward (Fig. 25).
If the patient cannot sit, then the examiner raises the leg at the knee joint so that the lower leg hangs freely, and then strikes the tendon.
The main condition for obtaining a reflex is that all the muscles of the leg are completely relaxed. Relatively often, this condition is not met: the patient keeps the antagonists tense, as a result of which the reflex is not evoked. Then resort to various artificial methods to eliminate this undesirable phenomenon. There are quite a few of these tricks; the most common are the following: the Iendrassik method. The patient crosses his legs and, bending the fingers of both hands with a hook, grabs them for each other and strongly stretches his arms to the sides; the researcher at this time causes a reflex. Shenborn method (Schonbom). The position of the patient is the same. The doctor holds out his left hand to him, makes him grab his forearm and squeeze it with both hands, while he right hand at this time causes a reflex. Kronig's method. During the study, the patient is forced to take a strong breath and look at the ceiling at this time. Rosenbach's method. Volnoy during the study is forced to read loudly or say something.
Sometimes, if all attempts to evoke a reflex fail, it is enough to make the patient walk around the room for several minutes, after which the reflex is already called (Kroner's method).
The reflex arc of the knee jerk passes at the level of three spinal segments: the 2nd, 3rd and 4th lumbar (L 2 - L 4), with the 4th lumbar playing the main role.
I will ask you to firmly remember the levels of each reflex, since this plays a very important role in the segmental diagnosis of diseases of the spinal cord.
The knee jerk is one of the most constant reflexes. Its absence, especially one-sided, usually indicates an organic disease of the nervous system. Only in the form of a very rare exception can be observed in completely healthy people such areflexia, and it remains doubtful whether they transferred to early age any disease associated with damage to the reflex arc.
To quantitatively measure the knee reflex, a number of bulky and impractical devices have been built that record on a rotating drum in the form of a curve the swings of the lower leg or the rises of the quadriceps muscle due to its contraction. So far, such an instrumental study has not yielded any special results.
As a rule, every specialist soon develops his own eye, which helps him to distinguish between gradations of reflexes. To designate these gradations, I advise you to use the following designations.
We are speaking - reflex is evoked when in terms of strength he does not represent anything special; live reflex, when there is a moderate increase; reflex increased, when there is undoubtedly a significant increase in the reflex.
A reflex change in the opposite sense is characterized as follows: sluggish reflex when there is a slight decrease in it; reflex is reduced when the weakening of it is very significant; no reflex when it is not possible to call it by any auxiliary methods.
The next most important tendon reflex is Achilles. In it, irritation of the Achilles tendon gives a contraction of the calf muscle.
It is called like this. The freestyle kneels on a chair so that the feet hang over the edge of the chair, and relaxes the muscles if possible. The examiner strikes the Achilles tendon with a hammer, resulting in plantar flexion of the foot (Fig. 26).
In bed, it is best to examine the Achilles reflex with the patient in the prone position. The doctor raises the patient's shin, holding the foot, which leads to a state of slight dorsiflexion. At the same time, the Achilles tendon is somewhat stretched, and a gift is applied along it with a hammer.
When the patient is on his back, the study is somewhat less convenient, since the blow with the hammer has to be done from the bottom up.
The inhibition of this reflex is much less pronounced, and therefore, as a rule, in practice it is not necessary to use any tricks to evoke it.
The Achilles reflex arc passes through the first and second sacral segments (S 1 - S 2), and the main role belongs to the first sacral.
The Achilles reflex is also one of the most constant. Most likely, every healthy person has it, like a knee, and its absence should be considered a pathological phenomenon. Regarding the sometimes observed absence of it in people who are obviously healthy, one can only repeat what I have already said about the knee jerk.
Quantitative characteristic the Achilles reflex, with the help of various instruments, gives even less than for the knee reflex, and therefore it is best to evaluate it as I already recommended to you when I spoke about the patellar reflex.
On the hands, most often you have to deal with two tendon reflexes - c m. biceps and with m. triceps.
Biceps reflex
It is called like this. the doctor takes the patient by the forearm, bends him at the elbow at an obtuse angle and hits the biceps tendon with a hammer. As a result, a single flexion at the elbow occurs (Figure 27).
This reflex is very constant, but still not the same as the knee and Achilles. Apparently, it can be absent in a certain percentage of cases or, which is practically the same thing, be expressed extremely weakly.
Its reflex arc passes through the fifth and sixth cervical segments (c 5 - C 6).
Triceps reflex consists in the contraction of this muscle from a blow to its tendon.
The way to call it is as follows: the doctor puts on his left hand the upper limb of the patient, bent at the elbow at an obtuse angle, and hits the tendon of the triceps muscle in the lowest part of the shoulder with a hammer. At the moment of impact, a single extension at the elbow occurs (Fig. 28).
With regard to this reflex, as well as the previous one, it can be said that it is very frequent, but apparently not absolutely constant, or may be extremely weakly expressed in a certain percentage of cases.
Its reflex arc passes through the sixth and seventh cervical segments (C 6 - C 7).
On the head, the most popular tendon reflex is reflex with m. masseter.
It is called like this: the patient is asked to open his mouth slightly, put the end of a wooden spatula on his lower jaw teeth, and hold the other end with his left hand. Then the spatula, like a bridge, is hit with a hammer. The mouth is closed.
You can cause the same reflex by hitting the hammer on the chin or at the place of attachment of the upper end of the masticatory muscle on the zygomatic bone.
Tendon reflexes also belong to their own, or proprioceptive, reflexes. A blow to the tendon causes stretching of the muscle and thereby excitation of the proprioceptors located in it. Thus, the tendon reflex, like the stretch reflex, is essentially a muscular reflex. A blow to the muscle itself cannot give the same effect in strength, since it causes stretching of only a limited number of muscle bundles, while a blow to the tendon acts on all muscle fibers. The tendon itself is not a source of a proprioceptive impulse, and during anesthesia of the tendon, the tendon reflex, as well as the stretch reflex, is preserved. To obtain a muscle's own reflex, a very slight stretching of it, measured in hundredths of a millimeter, is required.
In principle, the tendon reflex can be obtained from each muscle, but it is much easier to elicit from the extensor tendons, which have a large number proprioceptors - muscle spindles. Tendon reflexes have a short latent period, which is explained not only in a short reflex arc that transmits an impulse from sensory fibers directly to motor ones, without an intercalary neuron, but also in a thick caliber and, therefore, rapid conduction of the corresponding sensory fibers. A jerky blow to the tendon, causing a rapid stretching of the muscle, gives it a quick and short contraction. This tendon reflex differs from the stretch reflex in the proper sense, which is caused by prolonged passive stretching of the muscle. The tendon reflex is carried out by the phasic function of alpha cells without the participation of the gamma system.
Not all tendon reflexes have acquired clinical significance, but only those that are distinguished by constancy, or rather, greater clarity compared to many others that are in a latent state. As noted earlier, when entering the spinal cord, prioceptive impulses also propagate to neighboring, often distant levels of the spinal cord, but the shortest paths usually have clinical significance, the state of which can be judged by the results of the study of the corresponding reflexes. However, under pathological conditions, reflexes with a longer arc may become important. So, for example, in case of violation of the integrity of the effector part of the arc of the reflex of the biceps muscle of the shoulder, a blow to the tendon m. bicipitis can cause forearm extension instead of flexion. Such a paradoxical reflex is explained by the transmission of afferent impulses to the preserved motor pathways of neighboring segments. The paradoxical reflex is especially pronounced with a simultaneous increase in the excitability of the anterior horns due to the loss of inhibitory impulses from the central pathways. In the same way, a blow to the tendon of the quadriceps muscle can cause flexion of the lower leg rather than extension.
 Tendon reflexes may be absent, they may be decreased or increased. Absence or demotion speaks for the most part about the lesion in the area of the reflex arc: in the peripheral nerve - with neuritis, with muscular dystrophies, in the posterior roots - with a traumatic lesion, with radiculitis, or spinal meningitis, dorsal tabes, with tuberculosis or a tumor of the vertebra, etc., in the spinal cord - with myelitis, gliosis, hematomyelia in the region of the corresponding reflex segment, with acute or chronic poliomyelitis, some hereditary diseases such as Friedreich's ataxia. The absence of tendon reflexes has in clinical neurology great importance and is often the decisive symptom for a local diagnosis. But here it must be emphasized that the absence of tendon reflexes does not always make it necessary to localize the painful process in the region of the reflex arc. Knee or Achilles reflexes may sometimes be absent in brain disease - with tumors or dropsy of the head, causing an increase in intracranial pressure. More often this happens when a tumor (or abscess) is localized in the cerebellum. In such cases, the role and influence high blood pressure in the skull on pressure in the spinal canal, as a result of which the outgoing roots are damaged, and, perhaps, a toxic effect on the cells of the anterior horns, where the reflex arcs are closed.
Tendon reflexes may be absent, they may be decreased or increased. Absence or demotion speaks for the most part about the lesion in the area of the reflex arc: in the peripheral nerve - with neuritis, with muscular dystrophies, in the posterior roots - with a traumatic lesion, with radiculitis, or spinal meningitis, dorsal tabes, with tuberculosis or a tumor of the vertebra, etc., in the spinal cord - with myelitis, gliosis, hematomyelia in the region of the corresponding reflex segment, with acute or chronic poliomyelitis, some hereditary diseases such as Friedreich's ataxia. The absence of tendon reflexes has in clinical neurology great importance and is often the decisive symptom for a local diagnosis. But here it must be emphasized that the absence of tendon reflexes does not always make it necessary to localize the painful process in the region of the reflex arc. Knee or Achilles reflexes may sometimes be absent in brain disease - with tumors or dropsy of the head, causing an increase in intracranial pressure. More often this happens when a tumor (or abscess) is localized in the cerebellum. In such cases, the role and influence high blood pressure in the skull on pressure in the spinal canal, as a result of which the outgoing roots are damaged, and, perhaps, a toxic effect on the cells of the anterior horns, where the reflex arcs are closed.
A reflex is usually called the response of the body to conditions external environment or external irritation. These processes occur and are controlled by the activity of the nervous system.
But it should be borne in mind that reflexes are divided into different types that carry out various reactions in the body. So, reflexes are usually divided into superficial and deep. If the surface ones are responsible for a small number of reactions, then the deep ones, on the contrary, control most of them.
Examination of reflexes in neurology allows not only to determine the degree of the affected area of the central and peripheral motor neutron, but also the level of disorders in the spinal cord and brain. In neurology, reflexes are divided into reactions of superficial and deep types.
Superficial reflexes are responsible for the reactions of the skin, mucous membranes of the cornea of the eyes, and deep reflexes for the reactions of muscle fibers, periosteum, tendons, and joints. Deep reflexes are much more diverse and are responsible for multiple reactions in the body.
What are deep reflexes
Deep reflexes are considered to be involuntary muscle contractions that act as a response to a stimulus containing muscle spindle receptors. This process occurs in the form of involuntary muscle contractions with stretching of the tendons of a passive nature.
Often this type of stretching is determined during a small jerky blow at the place of attachment of the tendons to the muscles, which is carried out with a special neurological hammer. When determining the reaction, the patient should assume a relaxed state, tension and stiffness should be avoided.
In this case, all muscle tissues must be completely relaxed, otherwise it will be impossible to determine the presence and degree of a particular reflex. If the patient will experience tension in one or another part of the muscles, he will stretch the muscle, then the reflex will be inaccurate or disappear altogether.
If the reaction occurs with difficulty, then the doctor asks the patient to distract himself from the place under study, for example, when examining the reactions of the legs, he is asked to tightly clamp his teeth or interlock his fingers on both hands and pull his arms to the sides with an effort, this is called the Jendrasik technique.

Degree of detection deep reflexes usually evaluated on a point system:
- 4 points- maximally increased reaction;
- 3 points- lively, but at the same time it has a normal expression;
- 2 points- the reaction is evaluated, in which the severity is normal;
- 1 point– low;
- 0 points- complete absence.
The severity of reactions in healthy patients can vary greatly. Usually, reactions in the legs are highly pronounced and much easier to cause than reactions in the arms.
Not always a slight manifestation of bilateral type reactions may be evidence of a violation of the activity of the pyramidal nervous system, this reaction can also occur in healthy people who have a high degree excitability of the nervous system.
Tendon and periosteal reflexes
Deep reflexes are divided into several groups, namely:
- tendon reflexes are reactions of an unconditioned type, which are caused by hitting a special neurological hammer in place with the attachment of the tendon to the area of \u200b\u200bmuscle fibers. These are mitotic reflexes, because they are based on the process of stretching not of the tendons, but of the muscles, which occurs due to the stretching of the tendons.
- reflexes periosteal view are unconditional. Reactions of this type occur during muscle stretching, which occur in response to excitation of periosteal receptors. Reactions of this type are manifested when struck with a neurological hammer.
During the examination, it is necessary to take into account the degree of severity and symmetry of the reactions. Be sure to remember that the severity of fluctuations and symmetry in all people is individual and different. Equally, reflexes cannot manifest themselves in everyone, they can be brightly animated or, on the contrary, not very pronounced. If there is an asymmetry of reflexes, then this will be a sign of the presence in the body of an organic lesion of the central nervous system.
Types of tendon reflexes
One of the most informative tendon reflexes is Achilles. His call occurs during the impact of a neurological hammer on the area with the Achilles tendon. The result is contraction and flexion of the foot. The call of this reflex is carried out by several methods, namely:
- The patient must sit down. He sits on his knees on the surface of the couch or chair. In this case, the feet should hang freely
- The patient lies on the abdomen. During this, the doctor with his left hand should take both feet of the patient by the fingers and hold them at right angles to the lower leg.
- The patient must assume the supine position.. His leg should be bent at the large joints with its outward rotation. After that, the foot is bent in the back direction and a blow is made. During this procedure, a reaction occurs in the form of plantar flexion of the foot.
Other notable tendon reflexes:


Reflex arc of the knee jerk
Periosteal reactions
Periosteal (periosteal) reflexes:

During the examination of deep reflexes in the arm area, it is necessary to carefully examine the place with the spread of the reflex reaction. For example, if a carporadial reflex is called, then flexion of the fingers may appear, this process will indicate the presence of a lesion in the central motor neutron.
Sometimes there is an inversion or a process of perversion of the reflex - when instead of the biceps, the process of contraction of the triceps muscle of the shoulder is manifested. This disorder arises due to the spread of excitation to neighboring parts of the spinal cord, while the patient also has disorders in the anterior root, which intervenes the area of the biceps muscle.
During this process, a response motor reaction to this reflex should occur, which is accompanied by flexion and rotation of the arm at the elbow joint, while observed simultaneous flexion fingers.
TENDON REFLEXES- own (proprioceptive) unconditioned reflexes arising in response to stimulation of proprioceptors in a passively stretched muscle.
The main receptors for S. r. serve as sensitive end devices in the muscles - the so-called. neuromuscular spindles that respond to stretching of the muscle fibers caused by a blow to the tendon (see Proprioceptors). The receptors of the tendon itself do not play a significant role in the reflex, since the reflex can be obtained, for example, after local anesthesia of the reflexogenic zone or replacement of the tendon with an allograft. The afferent link of the reflex arc is sensitive thick A-fibers of the peripheral nerves and the posterior roots of the spinal cord. Reflex arcs S. p. close in the spinal cord (more often) or in brain stem. The beginning and end of the reflex arc are associated with the muscle.
Physiol. value S. r. consists in the fact that they, by regulating the degree of muscle contraction in accordance with the stimuli falling on it, participate in maintaining the statics and position of the body. Normal S. r. they are not exhausted, they change little from the summation of irritations, their refractory phase is short. The latent period of tendon reflexes is 6-20 ms. Speed S. r. associated with the simplicity of the structure of their reflex arc (in which there is usually one switch) and high speed conduction of excitation along nerve fibers.
Reflex arcs S. p. are under the influence of overlying departments of c. n. N of page, in particular a bark of a brain. It is known, for example, that when the knee jerk is induced, the electrical activity of the cerebral cortex changes. The nature of the reflex is affected by the posture of the body, the position of the limb under study, the functional state of other spinal centers that are not directly related to this reflex act.
Theoretically, S. p. there may be as many as there are muscles, but practically not all reflexes are equally accessible to research. The extensors of the lower extremities respond more easily to adequate stimulation, namely those muscles that resist gravity (anti-gravity). Adequate stimulation for tendon reflexes is stretching, pushing or hitting the tendon. When calling S. p. active muscle tension must be completely eliminated. You should always compare the reflexes on one and the other side. Highest value in a wedge, practice have the following S. of river.
Biceps tendon reflex(see Biceps reflex). Strike nevrol. hammer, applied to the tendon of the biceps muscle above the elbow, causes flexion of the arm in the elbow joint. The reflex is associated with the musculocutaneous nerve; its arc closes in the Su-Cvi segments of the spinal cord. In children, the reflex is caused from the first days of life.
Triceps tendon reflex(triceps reflex). To evoke a reflex, the shoulder of the patient’s relaxed arm is passively withdrawn outward to a horizontal level and the arm is supported at the elbow joint so that the forearm hangs at a right angle. The hammer is struck near the olecranon, since the triceps muscle has a very short tendon. A blow to the tendon of the triceps muscle causes contraction of this muscle and extension of the arm in the elbow joint. The reflex is associated with the radial nerve; its arc closes in segments C4-C7. In children, the triceps reflex is caused from the first days of life.
Patellar (or patellar) reflex(see Patellar Reflex): A blow to the tendon of the quadriceps femoris below the kneecap causes the leg to extend at the knee joint.
The reflex is associated with the femoral nerve; its arc closes in segments L2-L4. The knee jerk is caused in most newborns from the first hours of life. In young children, knee jerks are more pronounced than in adults.
Achilles reflex caused by a blow to the Achilles tendon, resulting in plantar flexion of the foot (see Achilles reflex). The reflex is associated with the sciatic nerve; its arc closes in segments L5-S1-2. The Achilles reflex is caused in about 40% of newborns.
Mandibular (or mandibular) reflex is a reflex from the masseter muscle. A blow with a hammer on the patient's chin (preferably on the phalanx of the finger applied by the doctor to the patient's chin) with a slightly ajar mouth causes contraction of the masticatory muscles and movement of the lower jaw upward, causing the jaws to close. The reflex is associated with the mandibular branch of the Vth nerve; the reflex arc of the reflex closes in the bridge; found in almost all healthy people.
Listed S. r. Normally, they are easily caused with a certain skill and knowledge of techniques that eliminate arbitrary delay of reflexes. S. r. on the arms and legs, as a rule, are uniform on both sides.
Change of normal S. of river. can manifest itself in their decrease or disappearance, which is usually associated with a violation of the integrity of the reflex arc in any of its departments. Besides, S. r. disappear with a sharp atrophy of the muscles due to the lack of contractile force in them; temporarily disappear S. p. (see. Areflexia) with an acute increase in intracranial pressure, as well as after an epileptic seizure, with a cerebral stroke and other conditions, with which there is a decrease in the excitability of the reflex apparatus of the spinal cord, temporary functional asynapsia (see Diaschiz, Reflex).
S.'s increase of river. occurs due to the "release" of the reflex arc from the descending influences of suprasegmental formations. At the same time, the zone, with which S. can be called, expands, clonuses of the hands, feet, kneecaps appear (see Clonus), as well as pathological, protective and other reflexes (see.
Bibliography: Bogorodinsky D.K., Skoromets A.A. and Shvarev A.I. Guide to practical training on nervous diseases, p. 5, M., 1977; Krol M. B. and Fedorova E. A. Main neuropathological syndromes, M., 1966; Multi-volume guide to neurology, ed. S. N. Davidenkova, vol. 2, p. 163, M., 1962; Khodos X. G. Nervous diseases, p. 135, Moscow, 1974; Brain W. R. Brain's diseases of the nervous system, Oxford - N. Y., 1977; aka Brain's clinical neurology, Oxford a. o., 1978; Monrad-Krohn G. H. The clinical examination of the nervous system, L., 1964.
When checking the condition of tendon, or myotatic (from the Greek. myos - muscle, tatis - tension), reflexes, a neurological hammer is used, which is applied with a short, jerky blow to the tendon of the muscle. This leads to its stretching, which is replaced by contraction, which is manifested by a response motor reaction. Muscle tone and tendon reflexes depend on the state of muscle spindles and afferent fibers. A blow to the muscle tendon stretches the muscle, irritating the spindles, and activates the afferent sensory neurons of the posterior horns, which transmit impulses to motor alpha motor neurons. The result is a muscle contraction, or myotatic reflex. The following tendon reflexes are usually tested. . The reflex from the biceps muscle of the shoulder (biceps reflex, flexion-elbow reflex) is caused by a blow of the hammer on the tendon of the muscle above the elbow bend or on its aponeurosis on the shoulder girdle, while the patient's arm should be half-bent and as relaxed as possible. Causing a reflex, the examiner places the patient's forearm on the substituted forearm of his left hand or supports the patient's hand by the hand. If the patient is sitting, then when checking this reflex, his forearms can lie freely on his hips. The examiner can, checking the reflex, feel the tendon of the biceps muscle of the patient with the thumb of the left hand, after which the blows with the hammer are applied to the nail phalanx of his thumb. The response when evoking a reflex is flexion of the forearm. The afferent and efferent parts of the reflex arc pass along the musculocutaneous nerve. The reflex arc closes in the C5-C6 segments of the spinal cord (Fig. 4.3a). . The reflex from the triceps muscle of the shoulder (triceps reflex, extensor-elbow reflex) is caused by a blow of the hammer on the tendon of the muscle above the olecranon, while the patient's arm is passively slightly retracted back and outward, the forearm in this case hangs freely. The response is the extension of the forearm. The afferent and efferent parts of the reflex arc pass through ulnar nerve. The reflex arc closes in the C7-C8 segments of the spinal cord (Fig. 4.36). Rice. 4.3. Examination of the reflex with the biceps (a) and triceps (b) muscles of the shoulder. The knee reflex (reflex from the quadriceps femoris muscle) is evoked in a patient in a sitting position (Fig. 4.4) or lying down (Fig. 4.5), by hitting the quadriceps tendon under the patella with a hammer, while the patient's legs are half-bent at the knee joints, left hand the examiner lies on the lower third of the hips of a seated patient or is brought under his knee joints if the patient is lying. The response is leg extension. The afferent and efferent parts of the reflex arc run along the femoral nerve. The reflex arc closes in the L2-L4 segments of the spinal cord. Rice. 4.4. Examination of the knee ref. 4.5. Examination of the patellar reflex in Lex in a seated patient. patient lying on his back. Chapter 4 The main motor cortico-muscular path. 87 . A reflex from the calcaneal tendon (Achilles reflex) is caused by a hammer blow on the calcaneal (Achilles) tendon (Fig. 4.6, a, b). If the patient lies on his back, then his leg can be passively bent by the examiner in the hip and knee joints and fixed in this position with his left hand. It is convenient to evoke a reflex in a patient kneeling, for example, on a chair, with dangling feet. The response is plantar flexion of the foot. The afferent and efferent parts of the reflex arc pass through sciatic nerve and its continuation - the tibial nerve. The reflex arc closes in the S1 and S2 segments of the spinal cord. . The mandibular reflex (mandibular reflex, reflex from the chewing muscle) is caused by a blow of the hammer on the lower jaw or on a spatula placed on the teeth of the lower jaw of a patient sitting with his mouth open. The response is the closing of the mouth. The afferent part of the reflex arc passes along the third branch of the trigeminal nerve (mandibular nerve), the efferent part of the reflex arc - along the motor portion of the same nerve. The reflex arc closes in the brain stem.